PAGES: [BACK to PROTEUS home page] Back to CKHS100 MAIN PAGE Outline Research protocol
SPECIAL TOPICS: Histograms/Central tendency Sensitivity/Specificity Rates Critical review
Evaluation Research Definitions Designs Sample size Sample methods Confounding
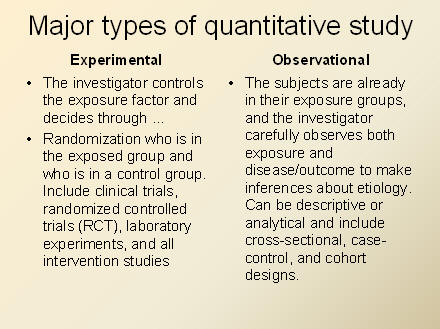
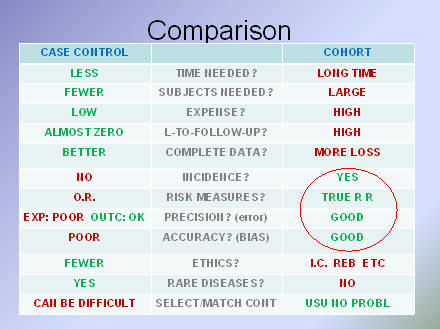
REMEMBER THAT IN CASE-CONTROL STUDIES (WHICH REALLY
SHOULD BE CALLED CASE-COMPARISON STUDIES), YOU START
WITH ILL AND WELL GROUPS AND GO BACK TO EXPLORE POSSIBLE
EXPOSURES.
IN COHORT STUDIES YOU START WITH HEALTHY EXPOSURE AND
NON-EXPOSURE GROUPS, AND FOLLOW THEM TO DISCOVER THE
INCIDENCE OF ILLNESS OVER TIME.
BUT IN A CASE-CONTROL STUDY YOU CAN NEVER "JOIN" THE ILL
AND WELL GROUPS FOR ANY REASON BECAUSE THEY ARE NOT
PROPORTIONAL TO EACH OTHER. HERE'S AN EXAMPLE.
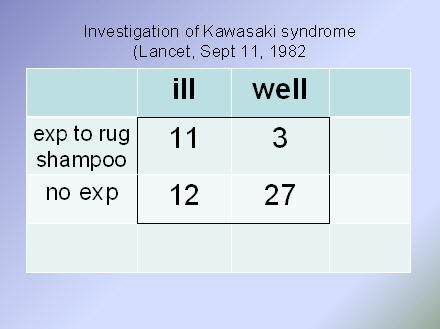
KAWASAKI SYNDROME IS A VERY RARE CONDITION. FEWER
THAN 1 IN A THOUSAND INFANTS ARE AFFECTED. SO IS IT
REASONABLE TO ASSUME THAT 14 (11+3) FAMILIES WHERE
CARPET SHAMPOO WAS USED WOULD SEE A CASE? OR THAT
12 OUT OF 39 FAMILIES WHERE NO CARPET SHAMPOO WAS USED
WOULD ALSO SEE A CASE? NO OF COURSE NOT. CASES AND
CONTROLS WERE ARTIFICIALLY SELECTED AND PLACED IN THIS
COMPARISON, AND WE CANNOT ASSUME "INCIDENCE RATES"
WHEN WE COMPARE CASE-CONTROL AND COHORT STUDIES, THE C-C SEEMS BETTER IN MOST CATEGORIES EXCEPT IN THE CONSISTENCY AND RELIABILITY OF DATA AND CONTROL OF BIAS (THE RED CIRCLE).